- Плоскостопие: виды, профилактика и лечение
- Причины возникновения плоскостопия
- Виды и степени плоскостопия
- Берут ли в армию с плоскостопием?
- Как определить плоскостопие, какой врач проводит диагностику
- Методы лечения плоскостопия
- Профилактика
- МОБИЛЬНОЕ ПЛОСКОСТОПИЕ У ДЕТЕЙ (ОБЗОР ЛИТЕРАТУРЫ)
- Полный текст
- Аннотация
- Ключевые слова
- Об авторах
- Владимир Маркович Кенис
- Юрий Алексеевич Лапкин
- Руслан Халилович Хусаинов
- Андрей Викторович Сапоговский
- Список литературы
Плоскостопие: виды, профилактика и лечение
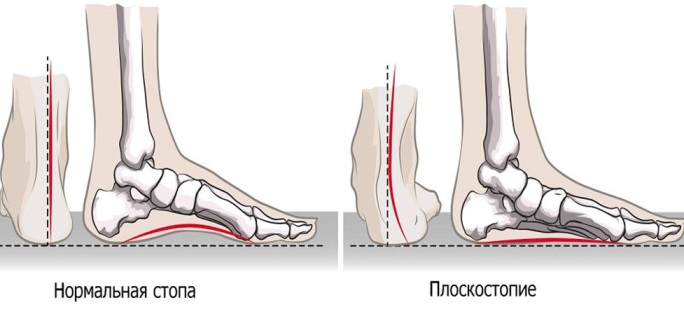
Плоскостопие у детей либо взрослых – это патологическое состояние, при котором вся подошва одной или обеих ног касается земли в положении стоя. Обычно внутренняя часть стопы (так называемый свод) немного приподнята над землей. При симптомах плоскостопия у взрослых, подростков либо детей практически нет свода или щели между кожей и полом. Плоскостопие влияет на осанку, может вызвать проблемы с лодыжками и коленями, что может изменить положение ног.
Причины возникновения плоскостопия
У маленьких детей свод обычно не виден из-за сильно развитых мягких тканей стоп и подкожно жировой клетчатки. С возрастом своды постепенно развиваются, формируя правильную постановку стопы.
Плоскостопие возникает по разным причинам, включая:
- травмы или повреждения сухожилия задней большеберцовой мышцы;
- генетическое наследование: плоскостопие может передаваться по наследству от родителей детям;
- проблемы с иннервацией: некоторые состояния, например, расщелина позвоночника, церебральный паралич или мышечная дистрофия, могут вызывать плоскостопие;
- врожденные нарушения: плоскостопие может возникнуть из-за аномалии, присутствующей во время рождения;
- неудобную обувь: ношение узкой или маленькой, жесткой обуви, высоких каблуков в течение длительного времени может вызвать плоскостопие;
- артрит или другие заболевания скелета.
Иногда чрезмерная нагрузка на стопу, мышечный дисбаланс, давление из-за веса тела также могут вызвать уплощение естественного свода стопы.
Виды и степени плоскостопия
Выделяют продольный свод стопы, который формирует арку с внутренней стороны от основания большого пальца до пятки, и поперечный, от основания большого пальца до мизинца. За счет сводов и подвижного сочленения костей стопа пружинит при ходьбе и смягчает удары. Соответственно, выделяют три типа патологии:
- поперечное;
- продольное;
- комбинированное (либо продольно-поперечное) плоскостопие.
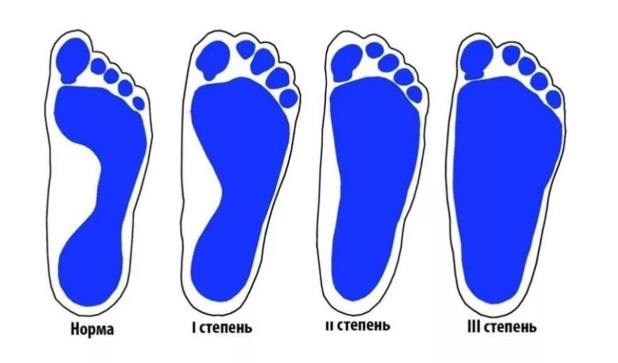
Кроме формы важно определение степени плоскостопия. От этого зависит тяжесть проявлений и лечение, развитие осложнений.
- 1 степень плоскостопия – нет деформации стопы, но ослаблены связки. Симптомы в виде дискомфорта или боли в ногах могут возникать при длительном пребывании на ногах, в вечернее время. После отдыха все они исчезают, возможно небольшое изменение походки.
- 2 степень плоскостопия – изменения стопы видны внешне, свод резко уменьшен, есть расширение и распластывание стопы. Боль в ногах достаточно выражена, возникает почти постоянно, распространяясь на голени. Походка изменена, возможно развитие косолапости.
- 3 степень плоскостопия – резко выражены изменения стопы, страдают суставы колена и бедра, позвоночника. Наблюдается деформация пальцев, постоянные боли в ногах, вплоть до бедер и ягодиц. Резко нарушена трудоспособность и походка, непродолжительная ходьба вызывает резкий дискомфорт, ношение обычной обуви невозможно.
Для поперечного плоскостопия выделена 4 степень, с высоким углом отклонения.
Берут ли в армию с плоскостопием?
Для юношей важен вопрос – с каким плоскостопием не берут в армию. По данным на 2020 год не берут в армию и не подлежат призыву парни:
- с поперечным либо продольным плоскостопием 2 степени, если выражен болевой синдром, есть деформация пальцев (артроз), контрактуры;
- продольное плоскостопие 3 степени, или поперечное 3-4 степени.
Они призываются только в военное время, получая на руки военный билет.
Как определить плоскостопие, какой врач проводит диагностику
Прежде всего, важны симптомы плоскостопия (у детей или взрослых), которые включают:
- боль в ногах;
- быстрое утомление ног, особенно в узкой обуви или на каблуках;
- боль в области сводов и пяток;
- отеки в нижней части стопы;
- затруднение и дискомфорт при стоянии;
- боль в коленях, бедрах и пояснице;
- деформация первых пальцев с формированием «косточек» по внутренней поверхности стоп;
- невозможность оторвать пятки от земли.
Кроме того, обувь снашивается с внутренней стороны, сильно деформируется. Все эти жалобы – повод для посещения ортопеда и диагностики плоскостопия.
Для выявления плоскостопия врач попросит встать на пальцы ног и опуститься на пол, посмотрит, касается ли ступня земли. Если врач заметит, что дуги нет или она слабо выражена, он порекомендует следующие тесты:
- Рентгенологическое исследование: рентген позволяет получить изображения костей и суставов стопы. Это также помогает выявить деформации суставов.
- Ультразвуковое сканирование: если врач подозревает какие-либо аномалии в сухожилиях, он порекомендует ультразвуковое сканирование. Это метод визуализации, при котором звуковые волны используются для создания изображений и визуализации поврежденного сухожилия.
- КТ: обследование с помощью компьютерной томографии помогает обнаружить травмы или переломы стопы и лодыжки. Он обеспечивает гораздо более подробные рентгеновские изображения, чем стандартный рентген при плоскостопии.
- МРТ: магнитно-резонансная томография дает более подробные изображения, чем ультразвуковое сканирование и компьютерная томография. В процедуре используются радиоволны и магнитные поля для получения изображений внутренних структур.
Методы лечения плоскостопия
Лечение плоскостопия зависит от симптомов и первопричины заболевания у взрослых либо детей. В некоторых случаях вмешательств не требуется, если состояние не вызывает боли или каких-либо других трудностей, не прогрессирует. Врач порекомендует конкретные варианты лечения, которые зависят от возраста и причин патологии.
Большинство случаев плоскостопия у детей являются генетическими. Однако их ступни гибкие от природы.
Исправление плоскостопия подразумевает:
- ортопедические стельки на заказ;
- соответствующую обувь, сшитую строго по размеру и особенностям ноги при плоскостопии;
- упражнения, курсы ЛФК;
- курсы физиотерапии;
- хирургический метод – зачастую это единственное лучшее решение для предотвращения серьезных осложнений развития в будущем, ели плоскостопие тяжелое.
Варианты безоперационного лечения для предотвращения развития плоскостопия и его симптомов у взрослых:
- Поддерживающие устройства для свода стопы. Врач порекомендует специально разработанные ортопедические устройства (стельки от плоскостопия), скобы или ортопедическую обувь для свода стопы, чтобы облегчить тяжесть при стоянии и ходьбе. Однако устройства поддержки свода стопы не излечивают болезнь, но помогают уменьшить симптомы.
- Физиотерапия. Физиотерапевт порекомендует определенные упражнения для облегчения боли, вызванной плоскостопием.
- Упражнения на растяжку. Врач порекомендует комплекс упражнений на растяжку, чтобы улучшить гибкость стоп при плоскостопии.

Кроме того, важна потеря веса, занятия физической культурой и полноценный отдых. Если безоперационные методы лечения не избавляют от болей, напряжения и проблем, связанных с плоскостопием, тогда следующим вариантом может быть операция.
Профилактика
Основные методы профилактики плоскостопия: регулярный осмотр ортопеда по мере взросления ребенка, подбор правильной обуви, физическая активность для гармоничного развития стопы. У взрослых это профилактика травм, контроль веса и подбор обуви по размеру и полноте стопы.
Источник
МОБИЛЬНОЕ ПЛОСКОСТОПИЕ У ДЕТЕЙ (ОБЗОР ЛИТЕРАТУРЫ)
- Авторы:Кенис В.М. 1 , Лапкин Ю.А. 1 , Хусаинов Р.Х. 2 , Сапоговский А.В. 1
- Учреждения:
- ФГБУ «НИДОИ им. Г. И. Турнера» Минздрава России
- ГБОУ ВПО «Северо-Западный государственный медицинский университет им. И. И. Мечникова» Минздрава России
- Выпуск: Том 2, № 2 (2014)
- Страницы: 44-54
- Раздел: Статьи
- URL:https://journals.eco-vector.com/turner/article/view/250
- DOI:https://doi.org/10.17816/PTORS2244-54
Цитировать
Полный текст
Аннотация
Ключевые слова
Об авторах
Владимир Маркович Кенис
Email: kenis@mail.ru
к. м. н., руководитель отделения патологии стопы, нейроортопедии и системных заболеваний
Юрий Алексеевич Лапкин
Email: omoturner@mail.ru
к. м. н., ведущий научный сотрудник научно-организационного отдела
Руслан Халилович Хусаинов
Email: drhuslan@gmail.com
аспирант кафедры детской травматологии, ортопедии и хирургии
Андрей Викторович Сапоговский
Email: sapogovskiy@gmail.com
врач отделения патологии стопы, нейроортопедии и системных заболеваний
Список литературы
- Болтрукевич С. И. Корригирующий латеральный артрориз подтаранного сустава для лечения нефиксированной формы плоскостопия у детей: инструкция по применению // Гродно. 2011. С. 32.
- Ефимов А. П. Клинически значимые параметры походки / А. П. Ефимов // Травматология и ортопедия России. 2012. 63. № 1. С. 60-65.
- Лапкин Ю. А., Кенис В. М. Варианты статической плоско-вальгусной деформации стоп тяжелой степени у детей / Материалы II Евразийского конгресса и II съезда травматологов-ортопедов Кыргызстана // Медицина Кыргызстана. 2011. № 4. С. 176.
- Садофьева В. И. Рентгено функциональная диагностика заболеваний опорно-двигательного аппарата у детей. Л.: Медицина, 1986. 240 с.
- Храмцов П. И. Функциональная стабильность вертикальной позы у детей в зависимости от свода стоп / П. И. Храмцов, А. М. Курганский // Вестн. Росс. акад. мед. Наук. 2009. № 5. С. 41-4.
- Aharonson Z. Foot-ground pressure pattern of flexible flatfoot in children, with and without correction of calcaneovalgus / Aharonson Z, Arcan M. Clin Orthop. 1992; 278:177-182.
- Basmajian J.V. The Role of Muscles in Arch Support of the Foot an electromyographic study/ J. V. Basmajian, G. Stecko. The Journal of Bone & Joint Surgery. 1963; 45:1184-1190.
- Bertani A. Flat foot functional evaluation using pattern recognition of ground reaction data/ A. Bertani [et al.]. Clinical biomechanics (Bristol, Avon). 1999; 14(7):484-93.
- Bleck E.E. Conservative management of pes valgus with plantar flexed talus flexible / E. E. Bleck, U. J. Berzins. Clin. Orthop. 1973;125: 85.
- Brewerton D.A. «Idiopathic» pes cavus: an investigation into its aetiology / D. A. Brewerton [et al.]. British medical journal. 1963; 2:659-661.
- Cavanagh P.R. The arch index: a useful measure from footprints / P. R. Cavanagh, M. M. Rodgers. Journal of biomechanics. 1987; 20(5):547.
- Chang J. H. Prevalence of flexible flatfoot in Taiwanese school-aged children in relation to obesity, gender, and age / J. H.Chang [et.al.]. Eur J Pediatr. 2010; 169(4):447-52.
- Christopher Rose R.E. Flat feet in Children: When should they be treated / R. E. Christopher Rose. Flat feet in Children: When should they be treated. 2006; 5(1).
- Cicchinelli L.D. Analysis of gastrocnemius recession and medial column procedures as adjuncts in arthroereisis for the correction of pediatric pes planovalgus: a radiographic retrospective study / L. D. Cicchinelli [et al.] J Foot Ankle Surg. 2008; 47(5):385-91.
- Cook D.A. Observer variability in the radiographic measurement and classification of metatarsus adductus / D. A. Cook [et al.]. Journal of pediatric orthopedics. 1992;12(1):86-89.
- Cowan D.N. Foot morphologic characteristics and risk of exercise-related injury/ D. N. Cowan [et al.]. Archives of family medicine. 1993;2(7):773-777.
- Dogan A. The results of calcaneal lengthening osteotomy for the treatment of flexible pes planovalgus and evaluation of alignment of the foot / A. Dogan [et al.]. Acta orthopaedica et traumatologica turcica. 2006;40(5):356-366.
- Echarri J.J. The development in footprint morphology in 1851 Congolese children from urban and rural areas, and the relationship between this and wearing shoes / J. J. Echarri, F. Forriol. Journal of pediatric orthopedics. Part B. 2003; 12(2):141-146.
- Ekcali O., Kosay C., Kaner B., Arslan Y., Sagol E., Soylev S., Iyidogan D., Cinar N., Peker O. Flexible flatfoot and related factors in primary school children: a report of ascreening study. Rheumatol Int. 2006; 26(11):1050-3.
- Evans A.M. The flat-footed child — to treat or not to treat: what is the clinician to do? / A. M. Evans. J Am Podiatr Med Assoc. 2008; 98(5):386-93.
- Forriol F. Footprint analysis between three and seventeen years of age / F. Forriol, J. Pascual. Foot & ankle. 1990; 11(2):101-104.
- Franklin J. Obesity and risk of low self-esteem: a statewide survey of Australian children/ J. Franklin [et al.]. Pediatrics. 2006; 118(6): 2481-2487.
- Garcia-Rodríguez A. Flexible flat feet in children: a real problem? / A. Garcia-Rodriguez [et al.]. Pediatrics. 1999; 103(6):84.
- Giannini S. Kinematic and isokinetic evaluation of patients with flat foot / S. Giannini [et al.]. Italian journal of orthopaedics and traumatology. 1992; 18(2): 241-251.
- Giladi M. The low arch, a protective factor in stress fractures: a prospective study of 295 military recruits / M. Giladi [et al.]. Orthop Rev.1985;14:82-84.
- Grady J.F., Kelly C. Endoscopic gastrocnemius recession for treating equinus in pediatric patients / J. F. Grady, C. Kelly. Clin Orthop Relat Res. 2010; 458(4): 1033-8.
- Gutiérrez P.R. Giannini prosthesis for flatfoot / P. R. Gutiérrez, M. H. Lara. Foot Ankle Int. 2005; 26(11): 918-26.
- Hamel J. Resection of talocalcaneal coalition in children and adolescents without and with osteotomy of the calcaneus. Oper Orthop Traumatol. 2009;21(2): 180-92.
- Harris R.I. Hypermobile flat-foot with short tendo achillis / R. I. Harris, T. Beath.The Journal of bone and joint surgery. American volume.1948; 30A(1):116-140.
- Hayashi B. Gastrocnemius recession: Effective remedy for recalcitrant foot pain / B. Hayashi [et al.] / http:// ww/aaas.org/news/bulletin/oct07/clinical4.asp
- Hefti F. Flatfoot / F. Hefti, R. Brunner. Der Orthopäde. 1999; 28(2):159-172.
- Hunt A.E. Mechanics and control of the flat versus normal foot during the stance phase of walking / A. E. Hunt, R. M. Smith. Clinical biomechanics (Bristol, Avon). 2004;199(4):391-397.
- Jerosch J. The stop screw technique— a simple and reliable method in treating flexible flatfoot in children / J. Jerosch, J. Schunck, H. Abdel-Aziz. Foot Ankle Surg. 2009;15(4):174-8.
- Kanatli U., Gözil R., Besli K., Yetkin H., Bölükbasi S. / U. Kanatli [et al.]. The relationship between the hind-foot angle and the medial longitudinal arch of the foot. Foot Ankle Int. 2006;(27)8:623-7.
- Keenan M.A. Valgus deformities of the feet and characteristics of gait in patients who have rheumatoid arthritis / M. A. Keenan [et al.]. The Journal of bone and joint surgery. American volume. 1991; 73(2):237-247.
- Kernbach K.J., Blitz N.M. The presence of calcaneal fibular remodeling associated with middle facet talocalcaneal coalition: a retrospective CT review of 35 feet Investigations involving middle facet coalitions. Part II / K. J. Kernbach, N. M. Blitz. J Foot Ankle Surg. 2008;47(4):288-94.
- Kilmartin T.E. The significance of pes planus in juvenile hallux valgus / T. E. Kilmartin, W. A. Wallace. Foot & ankle.1992;13(2):53-56.
- Koning P.M. Subtalar arthroereisis for pediatric flexible pes planovalgus: fifteen years experience with the cone-shaped implant / P. M. Koning, P. J. Heesterbeek, E. J. de Visser. Am Podiatr Med Assoc. 2009;99(5): 447-53.
- Kulcu D.G. Immediate effects of silicone insoles on gait pattern in patients with flexible flatfoot / D. G. Kulcu [et al.]. Foot ankle international. American Orthopaedic Foot and Ankle Society and Swiss Foot and Ankle Society. 2007;28(10):1053-1056.
- Lee J.H. Clinical or radiologic measurements and 3-D gait analysis in children with pes planus / J. H. Lee [et al.]. Pediatr Int. 2009;51(2):201-5.
- Leung A.K. A cross-sectional study on the development of foot arch function of 2715 Chinese children /A. K. Leung [et al.]. Prosthet. Orthop. Int. 2005;29(3):241-53.
- Levy J.C. Incidence of foot and ankle injuries in West Point cadets with pes planus compared to the general cadet population/ J. C. Levy [et al.]. Foot & ankle international. American Orthopedic Foot and Ankle Society [and] Swiss Foot and Ankle Society. 2006;27(12):1060-1064.
- Lin C.-J.J. Correlating Factors and Clinical Significance of Flexible Flatfoot in Preschool Children / C.-J. J. Lin [et al.]. Journal Of Pediatric Orthopedics. 2001;21(3):378-382.
- McPoil T.G. Effect of using truncated versus total foot length to calculate the arch height ratio / T. G. McPoil [et al.]. Foot (Edinburgh, Scotland). 2008;18(4):220-227.
- Meary R. On the measurement of the angle between the talus and the first metatarsal. Symposium: Le Pied Creux Essential / R. Meary. Rev Chir Orthop. 1967;53(389).
- Meary R. Symposium sur le pied plant / R. Meary. Ann Orthop Ouest. 1969;1:55-71.
- Mei-Dan O. The medial longitudinal arch as a possible risk factor for ankle sprains: a prospective study in 83 female infantry recruits / O. Mei-Dan [et al.]. Foot & ankle international. American Orthopaedic Foot and Ankle Society [and] Swiss Foot and Ankle Society. 2005;26(2):180-183.
- Menz H.B. Alternative techniques for the clinical assessment of foot pronation / H. B. Menz. Journal of the American Podiatric Medical Associa-tion.1998;88(3):119-129.
- Michelson J.D. The injury risk associated with pes planus in children / J. D. Michelson [et al. Foot Ankle Int. 2002; 27(7):629-633.
- Molayem I. Complications following correction of the planovalgus foot in cerebral palsy by arthroereisis / I. Molayem [et al.]. Acta Orthop Belg. 2009;(75)3:374-9.
- Mosca V.C. Flexible flat foot and skew foot / V. C. Mosca. Instr. Cource. Lect.1996;45:347-354.
- Mosca V.S. Flexible flatfoot in children and adolescents / V. S. Mosca. Journal of children’s orthopaedics. 2010;4(2):107-21.
- Murley G.S. Effect of foot posture, foot orthoses and footwear on lower limb muscle activity during walking and running: a systematic review / G. S. Murley [et al.]. Gait & posture. 2009;29(2):172-187.
- Nachbauer W. Effects of arch height of the foot on ground reaction forces in running / W. Nachbauer, B. M. Nigg. Medicine and science in sports and exercise. 1992;24(11):1264-1269.
- Nawoczenski D.A. The effect of foot structure on the three-dimensional kinematic coupling behavior of the leg and rear foot / D. A. Nawoczenski [et al.]. Physical therapy. 1998;78(4):404-416.
- Norman A.-C. Influence of excess adiposity on exercise fitness and performance in overweight children and adolescents / A.-C. Norman [et al.]. Pediatrics. 2005;115(6):e690-696.
- Pellegrin de, M. Subtalar screw-arthroereisis for correction of flat foot in children. Orthopade. 2005;34(9): 941-53.
- Pfeiffer M. Prevalence of flat foot in preschool-aged children / M. Pfeiffer [et al.]. Pediatrics. 2006; 118(2):634-639.
- Rao U.B. The influence of footwear on the prevalence of flat foot. A survey of 2300 children / U. B. Rao, B. Joseph. J. Bone Joint Surg Br. 1992;74(4):525-527.
- Redmond A.C. Development and validation of a novel rating system for scoring standing foot posture: the Foot Posture Index / A. C. Redmond [et al.]. Clinical biomechanics (Bristol, Avon). 2006;21(1):89-98.
- Redmond A.C. Normative values for the Foot Posture Index./ A.C. Redmond [et al.]. Journal of foot and ankle research. 2008;1(1):6.
- Rose G.K. The diagnosis of flat foot in the child / G.K. Rose [et al.]. The Journal of bone and joint surgery. British volume. 1985; 67(1):71-78.
- Rose Ch.R.E. Flat feet in children: When should they be treated? / Ch. R. E. Rose. Int. J. Orthop. Surg. 2007;6(1):1-10.
- Sachithanandam V. The influence of footwear on the prevalence of flat foot. A survey of 1846 skeletally mature persons / V. Sachithanandam, B. Joseph. The Journal of bone and joint surgery. British volume. 1995;77(2):254-257.
- Saltzman C.L. Measurement of the medial longitudinal arch / C. L. Saltzman [et al.] // Archives of physical medicine and rehabilitation. 1995;76(1):45-49.
- Scott G. Age-related differences in foot structure and function / G. Scott [et al.]. Gait & posture. 2007; 26(1):68-75.
- Shuen V. Acquired unilateral pes planus in a child caused by a ruptured plantar calcaneonavicular (spring) ligament. / V. Shuen, H.J. Prem. Pediatr Orthop B. 2009; 18(3):129-30.
- Smith M. A. Flat feet in children / M. A. Smith. BMJ (Clinical research ed.). 1990;301(6758):942-943.
- Soomekh D.J. Pediatric and adult flatfoot reconstruction: subtalar arthroereisis versus realignment osteotomy. surgical options / D. J. Soomekh, B. Baravarian. Clin Podiatr Med Surg. 2006;23(4):695-708.
- Sobel E. Natural history of the rearfoot angle: preliminary values in 150 children / E. Sobel [et al.]. Foot & ankle international. American Orthopaedic Foot and Ankle Society [and] Swiss Foot and Ankle Society. 1999;20(2):119-125.
- Staheli L. Corrective shoes for children: a survey of current practice / L. Staheli. Pediatrics. 1980;65:13-17.
- Staheli L.T. Planovalgus foot deformity. Current status / L.T. Staheli. Journal of the American Podiatric Medical Association. 1999; 89(2)94-99.
- Sullivan J.A. Pediatric flatfoot: Evaluation and management / J. A. Sullivan. J Am Acad Orthop Surg. 1999;7(1):44-53.
- Szczygiel E. Comparative analysis of distribution on the sole surface of arched feet and flat feet / E. Szczygiel [et al.]. Przeg. Lek. 2008;65(1): P. 4-7.
- Taunton J.E. A prospective study of running injuries: the Vancouver Sun Run “In Training” clinics / J. E. Taunton [et al.]. British journal of sports medicine. 2003;37(3):239-44.
- Tachdjian’s Pediatric Orthopaedics from the Texas Scottish Rite Hospital for Children. [ed. by J. A. Herring. 4-th ed.]. 2008.
- Templin D. The incorporation of allogeneic and autogenous bone graft in healing of lateral column lengthening of the calcaneus / D. Templin, K. Jones, D. S. Weiner. J Foot Ankle Surg. 2008;47(4):283-7.
- Thomas J.L. Radiographic values of the adult foot in a standardized population / J. L. Thomas [et al.]. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2006;45(1):3-12.
- Trzcinska D. Health school readiness of overweight and obese children against a background of peers / D. Trzcinska [et al.]. Pediatr Endocrinol Diabetes Metab. 2008;14(3):193-8.
- Vittore D.A. Extensor deficiency: first cause of childhood flexible flat foot / D. A.Vittore [et al.]. Orthopedics. 2009;32(1):28-35.
- Tudor A. Flat-footedness is not a disadvantage for athletic performance in children aged 11 to 15 years / A.Tudor [et al.]. lana.ruzic@kif.hr., PMID: 19254974 [PubMed — indexed for MEDLINE].
- Villarroya M.A. Assessment of the medial longitudinal arch in children and adolescents with obesity: footprints and radiographic study / M. A. Villarroya [et al.]. Eur J Pediatr. 2009; 168(5):559-67.
- Volpon J.B. Footprint analysis during the growth period / J. B. Volpon. Journal of pediatric orthope-dics.1994; 14(1):83-85.
- Vukasinovic Z. Flat feet in children /Z. Vukasinovic’ [et al.]. Srp Arh Celok Lek. 2009;137(5-6):320-2.
- Walczak M. Flexible flatfoot in children-a controversial subject / M. Walczak, M. Napiontek. Chirurgia Narzadow Ruchu I Ortopedia Polska. 2003; 68(4):261-267.
- Wan S.C. Metatarsus adductus and skewfoot deformity / S. C. Wan. Clin Podiatr Med Surg. 2006;23(1):23-40.
- Wearing S.C. The arch index: a measure of flat or fat feet? / S. C. Wearing [et al.]. Foot & ankle international. American Orthopaedic Foot and Ankle Society [and] Swiss Foot and Ankle Society. 2004; 25(8):575-581.
- Wenger D.R. Corrective Flexible Shoes and Inserts Flatfoot in Infants as Treatment for and Children/ D. R. Wenger [et al.]. The Journal of bone and joint surgery. 1989;71(6):800-810.
- Wrotniak B.H. The relationship between motor proficiency and physical activity in children / B. H. Wrotniak [et al.]. Pediatrics. 2006; 118(6):e1758-1765.

© Кенис В.М., Лапкин Ю.А., Хусаинов Р.Х., Сапоговский А.В., 2014
Эта статья доступна по лицензии Creative Commons Attribution 4.0 International License.
Источник


